Every year, thousands of women suffer life-altering injuries or die during childbirth because hospitals and medical workers skip safety practices known to head off disaster, a USA TODAY investigation has found.
Doctors and nurses should be weighing bloody pads to track blood loss so they recognize the danger sooner. They should be giving medication within an hour of spotting dangerously high blood pressure to fend off strokes.
These are not complicated procedures requiring expensive technology. They are among basic tasks that experts have recommended for years because they can save mothers’ lives.
Yet hospitals, doctors and nurses across the country continue to ignore them, USA TODAY found.
As a result, women are left to bleed until their organs shut down. Their high blood pressure goes untreated until they suffer strokes. They die of preventable blood clots and untreated infections. Survivors can be left paralyzed or unable to have more children.
The vast majority of women in America give birth without incident. But each year, more than 50,000 are severely injured. About 700 mothers die. The best estimates say that half of these deaths could be prevented and half the injuries reduced or eliminated with better care.
Instead, the U.S. continues to watch other countries improve as it falls behind. Today, this is the most dangerous place in the developed world to give birth.
Identifying every hospital that doesn’t provide recommended care is next to impossible. There is no national tracking system for childbirth complications. Mothers tell harrowing tales of survival, but they often have no idea whether their doctors and nurses did something wrong.
USA TODAY obtained more than a half-million pages of internal hospital quality records and examined the cases of more than 150 women whose deliveries went terribly wrong. Reporters contacted 75 birthing hospitals to track whether they follow recommended procedures.
Together, these documents and interviews reveal a stunning lack of attention to safety recommendations and widespread failure to protect new mothers.
At dozens of hospitals in New York, Pennsylvania and the Carolinas – where USA TODAY obtained records through federally funded quality programs – fewer than half of maternity patients were promptly treated for dangerous blood pressure that put them at risk of stroke. At some of those hospitals, less than 15 percent of mothers in peril got recommended treatments, the records show.
Many hospitals across the country conceded in interviews with USA TODAY that they were not taking safety steps such as quantifying women’s blood loss or tracking whether moms with dangerously high blood pressure got proper medication in time.
The lack of attention happens at hospitals big and small, from tiny community delivery units to major birthing centers that tout state-of-the art technology and training. It also happens in doctors’ offices when they miss or fail to act on signs of serious complications during pregnancy and after delivery.
In Ohio, Ali Lowry bled internally after giving birth in 2013, but medical staff didn’t recognize and act on the warning signs for hours, according to records in a lawsuit that she has since settled. By the time she was airlifted to another hospital for lifesaving surgery, her delivery hospital had nearly run out of blood and Ali’s heart had stopped.
In Texas, Beatriz Garcia nearly bled to death when doctors and nurses were slow to help her after not quantifying her blood loss, she alleged in federal and state lawsuits. Garcia’s heart stopped. She needed a hysterectomy. She’s now awaiting a kidney transplant.
And in South Carolina, one of the state’s top hospitals sent YoLanda Mention home with her newborn despite her dangerously high blood pressure. When she returned to the emergency room with even higher blood pressure and an excruciating headache, the staff made her sit for hours in the waiting room, according to a lawsuit filed by her husband. She had a stroke while waiting, and later died.
Today, YoLanda’s husband, Marco, is raising their three daughters alone in rural Nesmith. He balances work as a school bus driver with all the demands of raising kids on his own – cooking the meals, cleaning and getting three girls to schools and day care.
He spends his evenings leading his church choir and reminding his girls about a mother who the youngest knows as a picture in a curio cabinet.
“The girls, they ask when she’s coming home and I don’t know what to tell them,” Mention said, wiping tears. “It seems like a nightmare and I just need to wake up.”
It doesn’t have to be this way.
Countries around the world have reduced maternal deaths and injuries by aggressively monitoring care and learning from mistakes. The result has been two decades of steady or reduced maternal harms in the rest of the developed world – as U.S. rates climbed.
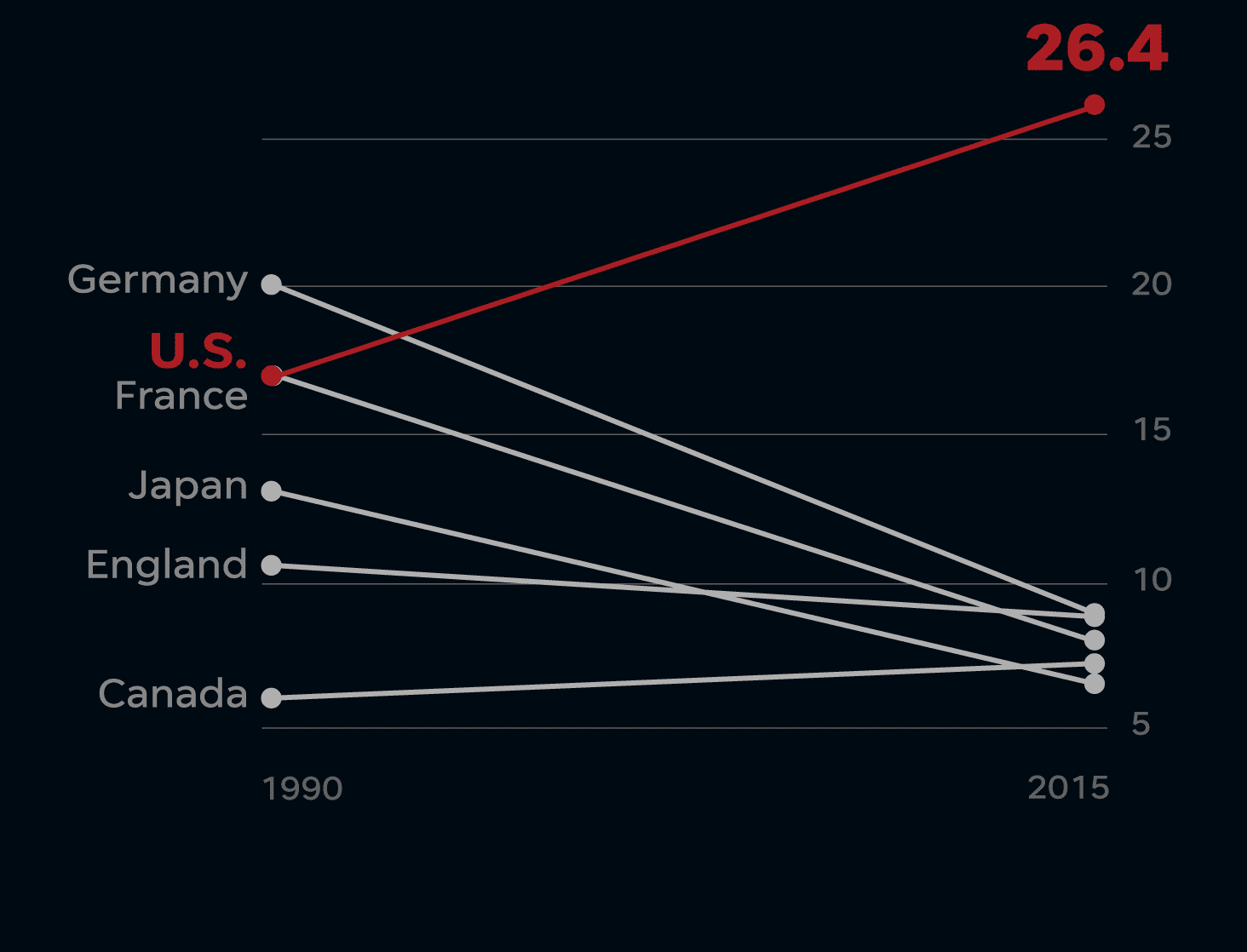
Divergent paths
From 1990 to 2015, the number of maternal deaths per 100,000 births in most developed nations has been flat or dropping. In the U.S., the rate has risen sharply.
One exception in the U.S.: California, where safety experts and hospitals worked together to implement practices that are now endorsed by leading medical societies as the gold standard of care. Statewide, California’s maternal death rate has fallen by half, while deaths rose across most of the country.
Despite widespread recognition that the California safety measures save lives, hospitals elsewhere have been slow to use them.
“Our medicine is run by cowboys today, where everyone is riding the range doing whatever they’re wanting to do,” said Dr. Steven Clark, a leading childbirth safety expert and a professor at Baylor College of Medicine. While there are hospitals that follow best safety practices, change is happening slowly, he said. “It’s a failure at all levels, at national organization levels and at the local hospital leadership levels as well.”
In part, that’s because regulators and oversight groups that could require hospitals to do more have not, USA TODAY found.
The lack of action by the Centers for Medicare and Medicaid Services to protect mothers stands in sharp contrast to its more aggressive approach to trying to improve care for elderly Medicare patients.
As a condition of getting Medicare payments, the federal agency requires hospitals to disclose information such as complication rates for hip and knee surgeries and whether heart attack patients got prompt care. All of that information is posted online.
That same agency helps pay for about half of the nation’s nearly 4 million births each year via Medicaid, and it could set similar rules about childbirth complications.
So far, it has not.
The Joint Commission, a private accreditation group that sets safety standards for thousands of hospitals, makes hospitals track cesarean section rates.
But the commission has no requirements that hospitals report how often their health care providers fail to follow national guidelines for protecting moms against leading childbirth dangers. Officials said the group is still studying the safety practices, some of which have been known for at least eight years.
“For us to make it a requirement for every organization to follow something, there has to be clear national consensus that this is the standard of care,” said Dr. David Baker, executive vice president of the commission’s Division of Health Care Quality Evaluation.
Baker said the safety practices to protect moms from hemorrhages are “promising.” But he said there are questions about whether the protocols calling for fast treatment of dangerous blood pressure are appropriate for the commission to require at the hospital level. “I suspect within the next two months, there will be a decision on whether to go forward,” he said.
The American Hospital Association, the influential trade association representing nearly 5,000 hospitals and health networks, has in recent years held closed-door training sessions aimed at getting maternity hospitals to improve care.
In a series of webinars, AHA first warned anyone not invited to disconnect.
Then, trainers for the association went on to bluntly discuss how wide-ranging care failures at birthing hospitals are causing needless deaths and injuries.
Secret training audio for medical staff
These recordings are from private training sessions held by the American Hospital Association for medical staff who deliver babies.
USA TODAY
“What we know about those deaths is that most of them were absolutely preventable,” a trainer for the association told maternity staffs during a 2015 webinar. “They were from causes that we could have done something about. We could have prevented it if we had recognized the emergency early on.”
During another closed session in 2016, a hospital association trainer said studies show that as many as 93 percent of women who bled to death during childbirth could have been saved if hospital staff had been aware of how much blood the woman lost.
The trainer said 60 percent of studied deaths from preeclampsia, a severe blood pressure disorder in pregnancy, also were preventable “because we failed to control the blood pressure or to recognize other emergencies that were happening.”
“We’re not talking about a Third World country, we’re talking about us, here,” the trainer said. “This shouldn’t be happening here.”
The hospital association declined to grant an interview and wouldn’t answer questions about the toll of preventable harms at its member hospitals or how many of those hospitals follow best practices. In a statement, the group said U.S. hospitals are “committed to continuously working to keep all patients safe.”
There is a growing recognition by hospitals that they need to adopt standardized care practices to save mothers’ lives. In the past year, the number of maternity hospitals participating in a voluntary childbirth safety improvement program endorsed by leading medical societies has more than doubled.
The 985 hospitals currently enrolled in the AIM Program to reduce harms to mothers represent about 40 percent of the nation’s birthing hospitals and they are in various stages of implementing care reforms, organizers say.
Routine failures
For more than a decade, the experts who guide medical practices in the U.S. have been pushing doctors and hospitals to change how they treat pregnant women.
At least as far back as 2010, researchers in California began promoting “tool kits” of childbirth safety practices to reduce deaths and injuries.
These kits, built upon years of published research, were made up of policies, procedures and checklists that, pursued together, appeared to save mothers’ lives.
Around the same time, the American College of Obstetricians and Gynecologists was lending its influence to address one of the leading childbirth killers: high blood pressure.
Help us report this story
We want to hear from you if you faced life or death complications — or felt you didn’t receive adequate care — during your pregnancy and childbirth.
Tell your story
In a 2011 bulletin to providers, the group warned that blood pressure above certain levels “if not treated expeditiously can result in maternal death.” The group gave hospitals and doctors step-by-step instructions, even specifying which IV drugs to give.
Three years later, a coalition of the nation’s leading medical societies created the AIM Program. The program formalized safety practices that have been shown to reduce maternal injuries into a series of “safety bundles” that detail treatment policies, safety equipment, training programs and internal reviews every maternity hospital should have.
The AIM Program’s “safety bundles” have been sponsored by a coalition of leading medical societies whose members include ACOG, the American College of Nurse-Midwives, the American Academy of Family Physicians and groups representing obstetric nurses and anesthesiologists.
For example, the AIM recommendations set time deadlines for taking blood pressure readings and administering medications to pregnant women and new moms experiencing dangerously high blood pressure.
Despite nearly a decade of medical studies, warnings, advice and training, hospitals continue to provide uneven care.
USA TODAY obtained internal hospital data collected from dozens of hospitals in 2015 and 2016 as part of other voluntary quality-improvement programs. Among other things, some of the federally funded programs tracked how often staff gave recommended blood pressure medicine within the called-for, one-hour deadline.
Among about 40 maternity hospitals in New York state, less than half of mothers experiencing dangerously high blood pressure got proper treatment, the records show.
In Pennsylvania, the data for about a dozen hospitals show mothers being promptly treated only 49 to 67 percent of the time.
More than 65 percent of mothers didn’t get proper treatment at Bon Secours St. Francis Hospital in Charleston, South Carolina.
At Carolinas Medical Center in Charlotte, North Carolina, nearly 40 percent of mothers did not receive timely blood-pressure treatments. The failure rate was 78 percent at Carolinas HealthCare System NorthEast in Concord and nearly 90 percent at Stanly Regional Medical Center in Albemarle.
At Alamance Regional Medical Center in Burlington, North Carolina, the breakdown was almost universal. Only one of the 48 maternity patients with dangerous blood pressure readings got proper treatment.
Officials at each of these hospitals said their performance has since improved.
Women’s Hospital in Greensboro is one of the biggest birthing hospitals in North Carolina, delivering about 6,000 babies a year in a metropolitan area of about 760,000 people.
The hospital says on its website “…whether you seek specialized care for a high-risk pregnancy, the latest diagnostic services, or alternative birth options such as a water birth, you can count on us for world-class service that’s close to home.”
But the federal records obtained by USA TODAY show doctors and nurses there put scores of mothers at risk by reacting slowly to signs of dangerously high blood pressure.
Women’s Hospital failed to provide timely blood pressure treatment for 189 of 219 mothers, according to its own monthly tallies from October 2015 through June 2016.
The treatment failures at Women’s Hospital occurred even though medical staff knew their work was being tracked.
Protect yourself
You can help protect your own life – or a loved one who is pregnant. This printable guide to take with you lists the most important questions you can ask the doctor and the hospital about their safety practices.
Get the Guide
“It’s unacceptable. That’s really what it is,” said Eleni Tsigas, who leads the Preeclampsia Foundation. She questions whether voluntary care-improvement programs alone will ever get enough hospitals to make lifesaving changes.
There is no way to know how widespread the failures like those in the Carolinas are at maternity units nationwide. The government doesn’t track it and hospitals’ internal numbers are usually a closely guarded secret.
Cone Health, which operates Women’s Hospital and Alamance Regional Medical Center, excused its poor performance in 2015-2016 by saying it had just started training staff to quickly treat dangerous blood pressure – even though ACOG issued its treatment warning in 2011.
Cone Health defended the delayed training by saying ACOG treatment guidelines aren’t mandatory and its own hospitals and doctors needed time to evaluate whether the best practices being touted by the nation’s top experts were appropriate.
The numbers suggest they were. Cone Health said its two hospitals that participated in the federal quality program have significantly improved.
At Women’s Hospital, 84 percent of mothers with high blood pressure got proper treatment from June 2016 to April 2017, officials said. At Alamance, it was 72 percent. And the number of mothers suffering seizures and strokes – consequences of dangerous, untreated high blood pressure – have dropped.
‘I was really scared’
It was about 4 a.m. when they wheeled Ali Lowry back to Room 25 at Knox Community Hospital after delivering her baby.
As a nurse in the hospital’s birthing center in Mount Vernon, Ohio, an hour northeast of Columbus, she had helped many other women deliver babies. But this was finally a baby of her own, and she was so excited to finally hold him.
As Lowry, 24, settled in and began breastfeeding her son, her vision went black.
“I was really scared, because I knew that, that I shouldn’t have been feeling that way,” she recalled of that morning in August 2013.
Lowry’s blood pressure had plummeted. Over the next hours, nurses took her blood pressure repeatedly and found it to be low. Around 5:30 a.m., the readings were: 52/26, 57/25, 56/24, 59/27.
Blood pressures at 85/45 or below ought to be a warning sign to hospital staff that a woman is losing life-threatening amounts of blood and action is needed, according to the childbirth safety tool kit California experts made available to hospitals across the country in 2010. For women like Lowry, who deliver by C-section, the bleeding can be internal and hidden from sight.
Yet for hours, no one at the hospital took emergency action to check for internal bleeding, according to records in Lowry’s lawsuit against her providers. Not the nurses on duty nor Dr. Ioanna Kanellitsas, who delivered Lowry’s baby. Instead, blood continued to pool inside her body and no one knew how bad it was.
It wasn’t until 7 a.m. – nearly three hours after she first began passing out – that the court records show Lowry started to get meaningful help to save her life.
A supervising nurse coming on duty saw Lowry’s blood pressure history and terrible condition, and mobilized a rapid response team. Lowry was moved to intensive care and started getting blood transfusions.
A doctor coming on duty, David De Lorenzo, found Lowry no longer lucid, her skin turning blue.
Around 10 a.m., Kanellitsas took Lowry into surgery and removed six cups of blood and clots from her abdomen. But she saw no active bleeding.
“We were in the operating room for an hour and a half watching this. So, I was as certain as I could be that we had controlled the bleeding and that she wasn’t having further bleeding,” Kanellitsas said in a deposition in the family’s lawsuit against the doctor and the hospital.
Yet Lowry kept bleeding. Unconscious and on a ventilator, blood soaked her legs and drenched her bed.
When nurses alerted Kanellitsas, the court records indicate the doctor told them it was OK. It looked like normal postpartum bleeding, she testified.
It is unclear whether the doctor and hospital staff had been quantifying Ali’s cumulative blood loss since her delivery. At least during Lowry’s C-section and later exploratory surgery, her blood loss – beyond what was collected in a suction machine – was being visually estimated, according to deposition testimony of the nurse anesthetist who was in the operating room for both procedures.
Multiple studies have found visual estimates underestimate blood loss, which can delay lifesaving treatments.
“She just kept getting worse and worse,” Ali Lowry’s husband, Shaun, said.
He had been asking for Ali to be transferred to a major medical center, but it refused to take her because she was too unstable.
By then it was clear that Lowry needed a hysterectomy to save her life – something Knox normally would have been able to handle.
But the hospital was down to its last unit of matching blood, according to court records. “We didn’t even have enough blood to give her a hysterectomy,” De Lorenzo said in a deposition.
De Lorenzo called Riverside Methodist Hospital in Columbus, which agreed to take Lowry.
As paramedics lifted her off the gurney, she went into cardiac arrest. If Lowry had stayed at Knox, De Lorenzo said: “She surely would have died.”
At Riverside, doctors found a lacerated artery, but had to remove Ali’s uterus to stop the bleeding.
“I was just kind of shocked by everything,” Lowry said. “I was definitely devastated by losing my uterus but at the same time I was also so thankful to be alive and that my baby was OK.”
The family settled a lawsuit against Kanellitsas and the hospital, who denied the suit’s allegations of wrongdoing. The terms are secret.
Knox officials declined to be interviewed. Frederick Sewards, an attorney for the hospital and Kanellitsas, said: “The resolution of that doubtful and disputed claim was subject to a confidentiality agreement, which neither I nor my clients will violate.”
Frustrations of the 50,000
Across the country, USA TODAY talked with dozens of women who are among the 50,000 each year who suffer severe injuries after surviving potentially deadly deliveries.
Some praise the care they received. But many women said they felt frustrated, angry and powerless after encountering doctors and nurses they felt didn’t listen or weren’t prepared for emergencies.
“This was supposed to be the best time of my life and this is the worst and nobody should feel that way about the birth of their child,” said Susan Goodhue of Annapolis, Maryland. Her blood pressure spiked and her liver and kidneys started to fail when she gave birth in 2012.
“The staff, by not knowing, and not listening and not taking precautions, almost killed us,” she said.
Women talked about excruciating pain and fighting to survive for their children. Some say they never got good explanations for what went wrong and why.
ZaKiya Bell-Rogers of Asheville, North Carolina, said she still doesn’t know what caused the blood loss that required her emergency hysterectomy in 2015. “I need to know what happened, but I don’t know if mentally I can take it if there was a mistake on their end.”
Donielle Bell, who lives in the Atlanta suburb of Marietta, also says she never got good answers about why she hemorrhaged in 2016 – and whether it would happen again when she gave birth to her third child this spring.
“I’m facing this fear daily,” she told USA TODAY earlier this year. “I’m terrified that I won’t walk away from it.”
In April, Bell delivered a healthy son, but she lost so much blood this time that she needed an emergency hysterectomy to save her life.
Over and over, these women said they wanted other mothers to know the importance of finding health care providers who listen to their concerns, pay attention to warning signs and are trained to deal with complications.
“Having the right hospital is life and death,” said Alana Alvarez of Mililani, Hawaii, who nearly bled to death and needed a hysterectomy and other surgeries to survive a 2015 birth.
“Having the right doctors, having the right care, having the right people that know about your diagnosis, that understand your diagnosis, that know what they’re doing, it’s life and death,” she said.
Attacking the problem
At University of Utah Hospital in Salt Lake City, maternity officials didn’t want to believe that the way they cared for mothers could be one of the reasons why 12 percent of their patients suffered hemorrhages in 2013 – triple the national rate.
Like many hospitals, they were quick to blame the women as being unusually high risk instead of scrutinizing their own care.
“We initially rationalized this,” Dr. Erin Clark, the hospital’s director for maternal-fetal medicine, told maternity staff from other hospitals at a 2015 training session.
But the hospital realized it had a problem when it compared its results with other university hospitals. Their peers also cared for high-risk moms, but their patients weren’t hemorrhaging as often.
“We stood out in an obvious way and not a good way,” she told USA TODAY.
The hospital dug into patients’ records. “We diagnosed hemorrhages too late,” Clark said. “And we didn’t treat them fast enough or aggressively enough.”
The hospital reduced its rate by one-third after it began adopting the best practices called for by California experts and the AIM Program, Clark said. That progress has been seen in other groups of hospitals following the safety practices, too.
According to a study published last year in the American Journal of Obstetrics & Gynecology, women giving birth in hospitals participating in a California quality-improvement collaborative suffered 21 percent fewer severe harms related to hemorrhage from 2014 through early 2016 than those in previous years. That’s fewer women suffering heart attack, kidney failure or blood-clotting disorders, and fewer women being put on ventilators or undergoing hysterectomies.
When hospitals work with well-organized state-wide quality groups – that help them train staff, track data and benchmark against peers – care can improve faster than if they’re left to do it on their own, experts said. From May 2016 through June 2017, about 100 Illinois hospitals participating in an AIM Program-affiliated project increased from 42 percent to 79 percent the number of maternity patients getting treatment for dangerous blood pressure within one hour, according to data published earlier this year in the same medical journal.
For decades, hospitals and medical experts have often blamed rising maternal deaths and injuries on women for being unhealthy or overweight, or pointed to risk factors such as poverty or the age of mother.
“Just because you’re older and heavier, doesn’t mean you should die,” said Dr. Elliott Main, medical director of the California Maternal Quality Care Collaborative, which is credited with reducing maternal injuries and deaths in the state. “That just means you should be on guard, you should bring your A game.”
Blaming moms for poor health or lacking prenatal care helps mask care failures.
“We cannot just blame the women,” said Debra Bingham, a former vice president at Association of Women’s Health, Obstetric and Neonatal Nurses, who is now at the University of Maryland School of Nursing.
Nurses and doctors believe they provide good care and don’t want to harm patients, Bingham said.
“So it’s very hard to accept that what I’ve been doing for years may not have been the best way to do it,” she said.
Women want answers
Until they had a birth go terribly bad, many women told USA TODAY they never knew different hospitals handle childbirth emergencies differently.
Rachel Yencha, who nearly bled to death after giving birth in 2015, said it would have been helpful to know upfront whether hospitals follow best safety practices.
Yencha, who was young and healthy, chose a small maternity hospital near her suburban Cleveland home. But when complications arose during delivery, she had to be transferred to a bigger hospital that could save her life.
“Even if you have a normal pregnancy, you want them to be prepared for anything,” she said.
Because there are no requirements that U.S. maternity hospitals follow best practices, nobody knows how many of them take all of the AIM Program’s recommended actions.
“I don’t have a good sense for what percentage of the hospitals. It’s not huge yet, but it’s gaining momentum rapidly,” said Dr. Barbara Levy, vice president of health policy at ACOG.
Even if women and their loved ones knew the questions to ask, USA TODAY found that it would be nearly impossible for them to find out the safety records of maternity hospitals or whether they are following best safety practices.
USA TODAY repeatedly contacted 75 hospitals in 13 states to press for specific answers about whether they are following the AIM Program’s recommended practices for hemorrhage and hypertension.
Half wouldn’t answer the questions.
Those refusing to answer included Northside Hospital in Atlanta, one of the nation’s largest birthing hospitals, which annually handles about 16,000 deliveries. “We are going to have to pass on this opportunity. I’m not able to get you what you need,” hospital spokesperson Katherine Watson said in an email.
“We respectfully decline to participate,” said Giselle Tiley, spokeswoman for Osceola Regional Medical Center in Kissimmee, Florida.
Even hospitals that brag about their expertise in childbirth emergencies wouldn’t answer questions about whether they are taking AIM’s recommended safety steps.
“We will pass on this one,” Johnny Smith, a spokesman for St. Agnes Hospital in Baltimore, said in an email after a reporter contacted the hospital and its parent health system, Ascension, nearly a dozen times. On its website, the hospital says: “Our innovative approach to obstetric emergencies set us apart.”
The 37 maternity hospitals that answered USA TODAY’s questions said they are doing many of the AIM Program’s best practices to prevent women from bleeding to death. But more than 40 percent acknowledged they were not quantifying blood loss after every birth – despite it being a cornerstone safety practice.
When it came to ensuring women with dangerous blood pressure readings got proper treatment within 60 minutes, the hospitals’ answers also indicated lax compliance. Of 31 hospitals that said they follow a 60-minute treatment policy, only nine said they track how often doctors and nurses actually gave treatment in time.
Experts say the slow pace of change is largely because, in this country, doctors and hospitals enjoy wide latitude in how they practice medicine. How they treat patients is often based on what providers were taught – years or decades earlier – in medical or nursing school, plus their individual experiences over time.
When researchers identify safer ways of caring for patients, there are no mandates that providers read or follow these practices. In maternity care – as well as other areas of medicine – it can take a decade or more for best practices to be widely adopted by health care providers.
The result: a system that experts say fails patients and leads to needless deaths and injuries.
In countries with publicly funded national health care systems, such as the U.K, it is easier to insist hospitals and health providers follow standard safety practices, said Dr. James Martin Jr., director of maternal-fetal medicine at the University of Mississippi Medical Center and a past president of ACOG.
Martin and other experts said that’s one reason why women giving birth in Great Britain die from childbirth complications at one-third of the rate they do here.
Without a centralized system, reform will require multiple entities to insist on change: hospital administrators, insurance companies and others that pay for childbirth, and malpractice insurers who defend practitioners against lawsuits, Martin said.
“If they say, ‘We expect you to do it this way,’ that you’ve got to get on and use this safety bundle … it can be driven from that point of view,” Martin said.
Hospitals need to be accountable and the public should be able to find out each hospital’s rates of childbirth complications, said Helen Haskell, president of Mothers Against Medical Error, a nonprofit patient safety group in South Carolina.
“We’ve put a lot of credence in the idea of voluntary improvement and it’s just not enough,” Haskell said. “You have to have transparency and you have to have regulation.”
Until that happens, women will continue to be harmed.
“So many of these are preventable,” said Monica Simpson, executive director of SisterSong, an Atlanta group that is part of the Black Mamas Alliance, which is pushing for national policy discussions. “I think the country should be outraged.”
The team behind this investigation
Reporting and research: Alison Young, Laura Ungar and Christopher Schnaars.
Editing: John Kelly and Chris Davis.
Photography: Jack Gruber, Liz Dufour, Alison Young and Mykal McEldowney.
Videos: Walbert Castillo, Lindley Taylor, David Hamlin, Chris Powers, Liz Dufour, Jack Gruber, Robert Lindeman, Alison Young, Mykal McEldowney, Laura Ungar, Lauren Herbert, Sarah Scanlan, Sam Upshaw, Erich Schlegelfor, Rob Deutsch, Daryl Bjorass, Romain Blanquart, Angeli Wright, Tanya Breen, Kelsey Kremer, Preston Mack, Susan Cohen, Angela Wilhelm and Robert Hanashiro.
Graphics and illustrations: Veronica Bravo, Mitchell Thorson, James Sergent, Ramon Padilla, Lindley Taylor, Merry Eccles, George Petras and Shawn Sullivan.
Digital production and development: Annette Meade, Craig Johnson, Evan Sundwick, Stan Wilson, Reid Williams, Mike Varano, Chris Amico, Kyle Omphroy, Eric Busch, Mitchell Thorson, Pim Linders, Josh Miller, and Shawn Sullivan.
Copy editing and design: Jeff Ruble, Susan Haas, Robert Abitbol, Rosalind Jackler and Ron Smith.
Social media, engagement and promotion: Anne Godlasky, Sean Rossman, Cara Kelly, Elizabeth Shell, Nichelle Smith, Emily Brown and Chrissy Terrell.